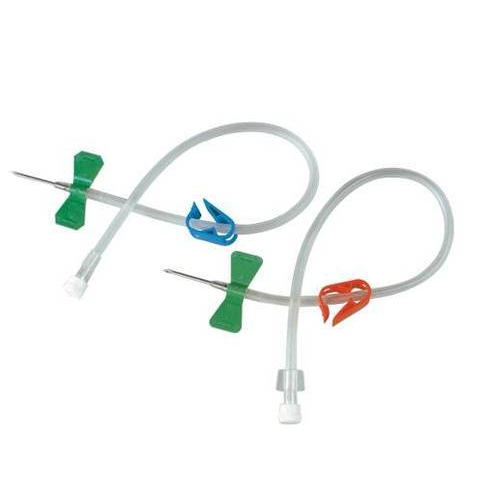
AV Fistula Needle
We feel proud to introduce ourselves as a manufacturer of AV Fistula Needle to our clients. Our offered needle is manufactured under the guidance of trained professionals using high quality raw material and modern techniques. Our offered needle is used during the dialysis to connect the blood lines to the blood vessels.
AV Fistula Needle
We feel proud to introduce ourselves as a manufacturer of AV Fistula Needle to our clients. Our offered needle is manufactured under the guidance of trained professionals using high quality raw material and modern techniques. Our offered needle is used during the dialysis to connect the blood lines to the blood vessels.
Features:
- Accurate dimensions
- Flexible wings for proper fixation.
- Safety Clamp available.
- Imported Japanese Cannula
- Imported Parts for Fistula.
Fistula needles are the crucial link between the patient and the dialysis machine. For this reason, all needles have to meet the requirements of highest quality, safety
and comfort – both from the user‘s as well as from the patient‘s perspective.
The strict quality control procedures incorporated during the manufacturing processes ensure the highest reliability and safety of fi stula needles from Fresenius Medical Care. Due to the ultra-thin walls of the needles, larger inner lumen diameter can be achieved, thereby permitting maximum blood fl ow rates. The strict quality control procedures incorporated during the manufacturing processes ensure the highest reliability and safety of fi stula needles from Fresenius Medical Care. All needles are equipped with a rotating wing and are coated with silicone to reduce the risk of bleeding and ensure optimal wound healing.
The amount of solute clearance achieved during dialysis is to a considerable extent determined by the effective blood fl ow rate. Fistula needles are the crucial link between the patient and the dialysis machine. For this reason, all needles have to meet the requirements of highest quality so av fistula needle.
Initially, these recommendations intended to be evidence-based. However, initial examination of the research indicated a wide variation in results, disagreement as to best practice recommendations from this research, and little relation to practical experiences of experts involved in developing the recommendations. Therefore, these recommendations are based on expert consensus opinion.
Contributors were encouraged throughout to discuss their own units practice and endorse recommendations that they would implement in their own unit, ensuring practical application of the recommendations. Co-authors were provided the opportunity to review and edit drafts of each section, to ensure agreement with the content. When practice was not agreed upon, options have been provided as to what could be best practice to include all opinions.
If needle insertion is not performed by the patient, prior to needle insertion, the ‘needler’ should discuss previous needling attempts with the patient. The patient should be encouraged to disclose their views on how to best insert the needle, how previous needle insertions progressed from their perspective and what may have caused previous problems,
The angle of insertion of the needle should be dictated by the minimum angle needed to reach the depth of the vessel to allow the needle tip to sit in the center of the vessel. This decision requires clinical judgment using the skill and expertise of the person inserting the needle.
Ideally, both needles should be inserted in an antegrade direction, with the needle pointing away from the anastomosis / with the flow of blood. If required, the arterial needle can be inserted in a retrograde direction, with the needle facing towards the anastomosis / against the flow of blood. This decision requires clinical judgment using the skill and expertise of the person inserting the needle.
Plastic cannulas to replace metal needles are a new innovation introduced to allow limb movement during hemodialysis, increase patient comfort, and reduce infiltrations. Some units are implementing plastic cannulas to minimize these complications. It is strongly recommended that service evaluations of using these cannulas, including patient experience measures, are performed. Units are cautious
of use, due to expense and unknown complications.
The pre-needle insertion assessment also ensures signs of complications are detected promptly. The look, listen, feel assessment can identify signs of infection, issues with skin integrity, signs of steal syndrome, and alteration inflow through the vessel indicating the development of stenosis. Detection allows prompt response to these signs, providing treatment of the complication before it escalates to a life-threatening issue or causes failure of the AV access.
As highlighted, the research base for needling techniques, especially that rope ladder is better than area puncture, is poor. Studies are needed to compare needling techniques. A comparison between buttonhole and rope ladder needs to be careful to ensure both techniques are performed correctly and consistently. Without this assurance, studies cannot claim to compare,
There are no maximum recommended times that decolonization should be undertaken,
however, twice is a common maximum number. Decolonization protocols should be pragmatic, taking consideration that hemodialysis patients may undergo these on multiple occasions.
Address
OPP AMBICA HOTEL,9 DIV 2,CTM,SHREE REVABHAI IND ESTATE,CTM, Opposite Shriji Hotel, Amraiwadi,
Ahmedabad-380026,
Contact Now
Mobile:- +919824041538
Email Us
beaconplastics@hotmail.com